
Why paediatric dentistry?

Children have had their own specialist physicians – paediatricians – for ages; in dentistry, there is now also an expert for children’s teeth: the paediatric dentist, also known as paedodontist.
Because a milk tooth is not merely a smaller version of an adult tooth, maintenance of milk teeth is extremely important for the correct development of the adult set of teeth; wrong treatment or their premature loss can lead to tooth and jaw problems with life-long consequences, the later correction of which may be laborious and complex.
In addition, our young patients have their very own special demands: Their fears need to be taken seriously; their treatment requires an ambience suitable for children and different methods than those for adults. The greatest requirement, though, is a great deal of patience, understanding and empathy in order to gain the children’s trust. Many adults suffer from a fear of dentists (dental phobia) for the rest of their lives, because they were traumatised as children by an unsympathetic and insensitive dentist. This must not happen!
For that reason, we are very happy that our team of experts is joined by an experienced dentist with an additional qualification in paediatric dentistry. When we built our new practice rooms it was our aim to realize a child-friendly ambiance with separate waiting and treatment rooms just for our little patients.
Topics
- Our paediatric dentist
- First consultation
- How we treat children
- How we treat milk teeth
- Prevention for children`s teeth
- The first teeth: Primary dentition
- Teething: What parents should look out for
- Fighting caries – From the very first tooth
- Dental trauma in children – What to do
- Chalky teeth – MIH
- Cleaning children’s teeth properly
- Preparing to the first visit to the dentist
- Questions and answers
Read or print a complete article on one page: Pediatric Dentistry in Lucerne: 
Video (in German):
Our paediatric dentist

Our paedodontist
is an experienced paediatric dentist. She genuinely enjoys working with children. She is particularly empathetic with the needs of anxious patients aiming to build trust and make a positive experience out of the treatment.
What parents write us (reviews)
At this point, we publish letters we received from the parents of our little patients.
Claudia Lombardi, Rotkreuz
The pediatric dentist is very empathetic and is very responsive to the child. Each step is announced and described in advance. The care is excellent. The child is distracted during the treatment by a funny movie. And most importantly, waiting and treatment rooms are designed for children..
Mira Dubroff, Luzern
Very nice and geared towards children. My daughter thought it was great and will like to come back without fear.
J.G., Oberkirch
The pediatric dentist explained and showed my daughter at the crocodile what she wants to do with her. She understood her understandingly. As a mother, the procedure was explained and my questions answered simply and clearly. The patching of the holes was painless and fast on the stage, so very different than I know it. The encouragements, the praise and the cartoon made everything even easier. The “Gschänkli” afterwards pleased her. The visit to the dentist is now a happy event for my children.
Yvonne Wey-Buchmann, Horw
Our Severin was lovingly received and with the introduction / explanation with the crocodile fears were reduced. We have received an informative brochure and recommendations. Thank you very much. We look forward to the next visit to the dentist.
Jamie Wenger, Roggwil BE
My daughter had to pull a tooth. I never thought that everything would be so relaxed. My daughter was totally relaxed and had no pain. Many thanks to the great dentist, who was amazingly sensitive and friendly. Thanks also to the great assistant.
The first appointment with the pediatric dentist

The purpose of the first visit is to allow the child to meet our paediatric dentist and see our dental practice and to develop trust in this new environment.
To ensure a positive first impression, we have made every effort to create a child-friendly ambience for our young patients in order to introduce them to dental treatment in a playful way.
With attention to detail and small gifts, we want to make sure that the child has good memories of this first contact with the paedodontist and feels positive about coming back.
For that reason, there should ideally be no actual treatment at the first appointment. However, the paediatric dentist will have an opportunity to get to know the young patient and to assess his treatment needs. This comprehensive examination also allows the experienced paedodontist assess the child’s willingness to receive treatment.
During the planning of the upcoming treatment, the children’s dentist can discuss with the parents whether the use of sedatives (sedation) or laughing gas may be advisable for a nervous, fearful child. If it can be foreseen that a child will refuse treatment altogether, it can be carried out under general anaesthetic.
The examination will also show whether poor nutrition may have been the cause of dental damage in the child and whether the parents might require nutritional advice. Prophylactic treatment for children may help in learning proper techniques for brushing teeth. Orthodontic treatment (braces) may be required to treat misalignments of teeth or jaws (dysgnathia).
Please download the registration form for children and return the completed form at your first visit.

Diagnosis
Diagnosis: Detecting dental decay – Modern caries diagnostics for children

Unfortunately, even today far too many milk teeth fall victim to caries. However, maintaining milk teeth is crucial for the unimpaired development of the permanent teeth. For that reason, the early detection of caries damage to milk teeth is important, while it is still limited and has not yet affected the nerve (pulp). Once a cavity in the tooth has become painful, it is often too late for a filling. In addition to the usual visual examination of milk teeth, we employ the following methods in the diagnosis of caries:
- X-ray
- Laser diagnostics
- Transillumination
- Assessment of caries risk
X-ray

It is a known fact that up to 70% of all caries damage to milk teeth is only detected in the early stages by X-ray. Our state-of-the-art digital X-ray appliances produce a very low radiation exposure and thus are particularly suitable for children.
When is an X-ray examination advisable for children?
- For new patients, it may be advisable in some instances to obtain a dental panoramic radiograph (orthopantomography or OPG) in order to get a picture of the child’s dental development and to rule out any developmental disorders.
- For children prone to caries: two annual intraoral bitewing radiographs.
- From age 3: annual check-up of interdental spaces with a bitewing radiograph
Laser cavity detector (Diagnodent)

This new non-invasive procedure is based on a laser beam whose reflection in the tooth is measured and evaluated by an electronic sensor. Scientific studies have confirmed a high success rate in the detection of hidden cavities.
Trans-Illumination

In this procedure, a strong light is shone through the tooth. If caries is present in the interdental space, the refraction of the light changes and a dark spot appears.
Assessment of caries risk
The caries risk of a child depends on a number of factors:
- Dietary habits (particularly foods containing sugar and carbohydrates)
- Cleaning habits (how often and how thoroughly)
- Saliva consistency and composition
- Bacterial activity in the mouth
- Surface structure of the teeth (quality of dental enamel, depth of grooves and pits in the enamel)
- Use of fluoride
In some cases, specific tests on the saliva can provide insights about individual caries risks.
How we treat children

Our foremost aim is for our young patients to be treated without fear or pain. In that way, we build up trust and prevent traumatisation as the result of negative impressions and experiences. This requires experience, patience and empathy.
At the same time, we try to make children feel positive about their treatment thanks to a child-friendly ambience. The kids can play in peace in the children’s waiting room. During treatment, we try to distract children from what is actually happening with age-appropriate toys and funny videos.
We also use special terms to explain to children what is going on without frightening them.
For example, a tooth does not get an “injection” but “sleep water” and goes to sleep; it is not a “drill” but a “tooth spray” that makes it clean and white, and so on.

We request that parents support us in this effort and do not talk at home about dentists in frightening terms.
To make sure that children are not disappointed in their trust, we need to make sure that their treatment is gentle and painless. For example, prior to the local anaesthetic, the paediatric dentist will apply a pleasantly tasting anaesthetic gel to the mucous membrane which allows a pain-free insertion of the needle.
Our experienced paediatric dentist is generally able to assess after the first appointment whether a child can be treated “normally” or has limited willingness to undergo treatment.
We offer special treatment methods for nervous or fearful children:
- Treatment with laughing gas and sedatives
- Treatment under general anaesthetic
The purpose of using these methods is twofold: it permits even particularly anxious children to be treated without stress. At the same time, it enables the children’s dentist to work more carefully on a sedated patient than on children who continuously wriggle and move, close their mouths and swallow.
Laughing gas – Magic air for young patients

Nitrous oxide was “discovered” more than 150 years ago by an American dentist and has since been used widely in medicine for sedation. Nowadays, laughing gas is regarded as the safest sedative in dentistry; dangerous events or complications can be practically ruled out with proper use.
The child is fitted with a small nasal mask and breathes a mixture of nitrous oxide and oxygen which can be adjusted by the paediatric dentist. The effect sets in after only a few breaths:
- The child is suffused with a warm feeling of well-being and security.
- What is happening with the treatment seems a long way away.
- Minor pain, such as the injection of local anaesthetic, no longer registers.
- Defence and swallowing reflexes are significantly reduced.
The child remains awake at all times, does not fall asleep during treatment, but experiences it in a positive light. At the end of the session, the patient is given pure oxygen for a few minutes to ensure that the nitrous oxide is fully eliminated and does not remain in the body. After only a few minutes, the child is fully “back to normal”. That is a great advantage compared with other sedatives that continue to affect the patient for hours afterwards and that require particular precautions.
Laughing gas and sedation – not suitable for all children!
Unfortunately, some limitations apply regarding the use of nitrous oxide in children. Children need to have a certain maturity and rationality to ensure a successful treatment. In general, laughing gas is not suitable for children who
- are unable consciously to breathe through their nose for extended periods of time (from age 5-6),
- have no insight into the necessity of treatment or who may even reject treatment.
Detailed information about treatment with nitrous oxide is available here.
For younger anxious children not suitable for treatment with laughing gas, the use of sedation may make sense. These sedatives can be administered as a suspension, a suppository or a nasal spray. The effect sets in after about 15 minutes. The child becomes sleepy and no longer registers stimuli from his/her surroundings. The disadvantage is that the effect of these sedatives continues for several hours beyond the actual treatment time and that children require close supervision by their parents during that time.
However, there are quite a few children who refuse dental treatment even after the administration of high doses of sedatives. The only alternative for these “total refuseniks” is treatment under general anaesthesia.
General anaesthetic: Sweet dreams
For very small and for particularly anxious children who do not yet understand the necessity of dental treatment, there is generally no alternative to treatment under general anaesthetic.
The Dental Team Lucerne has for years worked closely with experienced anaesthesiologists from narkose.ch. These specialists employ state-of-the-art and very safe anaesthetic procedures. Nausea after treatment, once a common feature of total anaesthesia, hardly occurs now; only a few minutes after treatment, the child is once again ”right as rain”. Under general anaesthetic, it is possible to treat an entire set of milk teeth in a single session, which may be an advantage for patients travelling from afar.
Detailed information about treatment under general anaesthetic is available here.
How we treat (milk) teeth
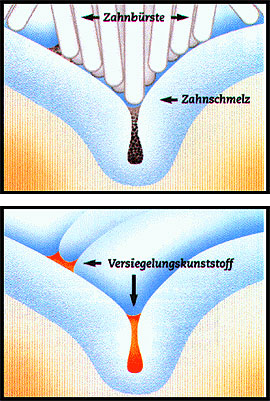

right: Fissure decay
Caries has a tendency to develop in the dental fissures, i.e. the grooves and pits on the chewing surface. This is also known as fissure decay.
To prevent this problem, the fissures in the teeth can be sealed with a liquid synthetic sealant, hardened by a special light.
If caries has already developed on the chewing surface, extended fissure sealing is used: the caries is gently removed with the drill, the defect filled and the chewing surface then sealed.
However, the latest recommendation is no longer to seal all teeth across the board. If a child is particularly prone to caries or has particularly deep dental fissures that make cleaning difficult, sealing of teeth still remains an advisable preventive treatment for dental decay. In fact, both milk and adult teeth can be sealed. However, sealing only protects the chewing surface of a tooth; the interdental space, also at high risk of caries, cannot be sealed.
Fillings
Milk teeth and permanent teeth are mainly affected by three types of caries:
- Occlusal (fissure) caries in the deep fissures and pits of the masticatory surface
- Approximal caries in the hard-to-reach interdental (approximal) space
- Smooth surface caries in the front and rear smooth walls of the teeth mainly develops in children as the result of poor nutrition, e.g. sugary drinks in feeding bottles.
Fillings in both milk teeth and permanent teeth are now generally made from tooth-coloured (white) materials which, if applied correctly, can last permanently. That is very necessary if you consider that children often only lose the last of their milk teeth at the age of 13.
The following materials are used in fillings:
- Composite fillings: The high-quality synthetic resin used for permanent teeth is also good for milk teeth. Composite is tough, durable and also suitable for larger defects.
- Compomer fillings: Compomer fillings are less mechanically stable than composites and are mainly used to fill smaller defects in milk teeth.
- Glass ionomer cement filings: Glass ionomer cement formulations stand out for their ease of use. However, in terms of life expectancy, they cannot compete with compomer or composite fillings. For that reason, their use is limited to temporary fillings and to milk teeth not expected to remain in the child’s mouth for any length of time.

Milk tooth crowns
Because the premature loss of baby teeth can cause lasting impairments to the development of permanent teeth (lack of space), it is very important to preserve the baby teeth.
A baby tooth crown is used if a milk molar has already been damaged by caries to such an extent that a normal filling is no longer an option. Crowns protect teeth from caries and stabilise them mechanically.
Thanks to crowning, the milk molars with their important role as place holders for the permanent teeth can generally be preserved for many years.
When is a milk tooth crown indicated?
- In cases of advanced caries when a normal filling is no longer an option.
- For milk molars after root treatment.
- In case of enamel defects (enamel malformations), in order to protect the tooth from caries.

Steel crowns are particularly durable and used in the back of the mouth on milk molars. Children rarely seem to be disturbed by the metal appearance – on the contrary, many kids consider it “cool”.

White crowns are steel crowns coated with resin or made completely from resin. They are more suitable for the front teeth (incisors) and guarantee a metal-free smile.
Root canal treatment of milk teeth
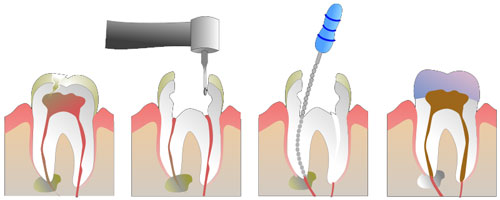
Treatment of the nerve or root of a tooth is always necessary if the dental nerve (pulp) is inflamed or necrotic (dead). As caries tends to progress quickly in comparatively soft baby teeth, the nerve is soon affected, which generally becomes noticeable through pain or discomfort.
Very often a small painless fistula develops at the edge of the gum with the appearance of a small blister, sometimes with a small discharge of pus.
Regrettably, even today many milk teeth that could easily be saved by root treatment are extracted far too quickly because of caries or fistulas
Milk tooth root treatment is used if
- Deep caries has penetrated to the nerve (pulp).
- The tooth has died as the result of an accident.
During root treatment – naturally under anaesthetic – the entire affected dental nerve (pulp) is removed and the root canal enlarged, cleaned and filled with special root cement.
If the caries has already reached the nerve, but the nerve is still healthy (no inflammation, no pain), it is generally sufficient for milk teeth to remove the upper part of the dental nerve (crown pulp). The remaining nerve in the roots is covered with a medicated filling and remains vital, i.e. is not killed. This procedure is known as pulpotomy.
Milk molars are ideally fitted with a milk tooth crown after root canal treatment for protection, in order to prevent them from breaking.
Treatment options
Despite all the treatment options available, it is not possible to save all milk teeth destroyed by caries. The premature loss of a baby tooth results in thedisplacement of teeth and a lack of space when the permanent teeth come through. This can lead to misalignments in the permanent teeth which necessitate elaborate correction with dental braces.
To prevent this, it makes sense in many cases to replace an extracted milk tooth with a place holder. This place holder assumes the function of the lost tooth and keeps the space for the permanent tooth. In this way, the gap is stopped from narrowing, thus allowing a smooth transition to the permanent dentition.
Place holders can be fixed (attached to the neighbouring tooth) or removable, like removable braces. Our paediatric dentist is happy to advise on the best place holder solution for your child.
Orthodontics
While these days most orthodontic treatment with braces is only performed during the latter stages of the mixed denture, from about the age of 12, there are some particularly serious misalignments of teeth and jaws that need to be diagnosed and treated in infancy.
Source: Austrian Board of Orthodontists (VÖK)
The misalignments of teeth and jaws can be congenital, but quite often are the result of bad habits. It may look sweet when babies suck their thumbs, but the result can be severe developmental impairments affecting teeth and jaws, such as open bite, crossbite, protruding teeth or a narrow jaw. In addition to thumb-sucking, there are other harmful habits such as the consistent insertion of other fingers or foreign bodies into the mouth or permanently pressing the tongue against the teeth.

Sucking habits should be stopped once the child has reached the age of three in order to prevent later and lasting damage.
A paedodontist can recognise such maldevelopments and initiate early treatment. Treatment consists of simple removable devices such as a vestibular plate.

The vestibular plate looks a little bit like a baby’s comforter and is used for early orthodontic correction. Its purpose is to stop children from sucking on their thumbs or a dummy. In addition, when fitted with an oral screen, it can also prevent the tongue from being pressed through the teeth. An open bite caused by sucking can thus be easily treated.
In difficult cases or for older children, treatment can also be administered by our orthodontic specialists in the Dental Team Lucerne who are expert in dental braces for school children, adolescents and adults. For school-age children, it is always advisable to visit the orthodontic specialist for a check-up.
Prevention for children’s teeth
Prevention for children′s teeth

We want our young patients to enjoy good teeth and healthy gums throughout their lives. The prerequisite for this target is perfect oral hygiene from a very early age.
In cooperation with our dental hygienists and dental prophylaxis assistants, our paedodontist has developed special prophylaxis programmes for children. In a manner understandable to them and appropriate to their age, children are shown the best way to clean their teeth. For children prone to caries, a saliva test can be used to determine their caries risk. In addition, the tooth enamel can be hardened using a fluoride varnish.
The first teeth
The first teeth: primary dentition
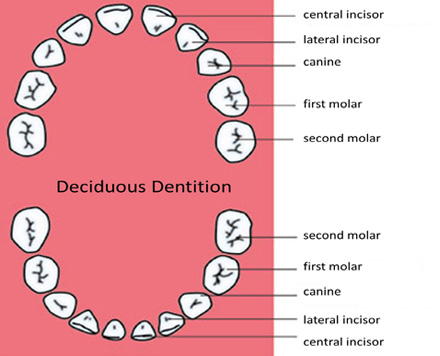
The jaws of babies and infants are not yet big enough to accommodate the permanent teeth. For that reason, humans, like many mammals, initially develop a deciduous dentition with 20 milk (deciduous) teeth.
There are 10 deciduous teeth per jaw: 4 incisors, 2 canines (eye teeth) and 4 molars. The milk teeth are smaller than the 32 permanent teeth that replace them later (second dentition).
When do the first teeth appear and when do they fall out?
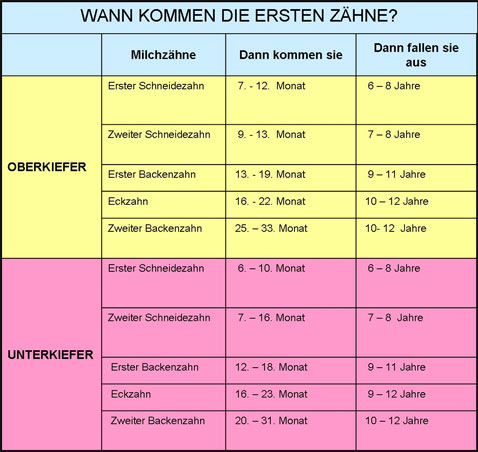

The first baby tooth to break through the mucous membrane at around 6 months of age is generally the lower incisor. The order in which the baby teeth appear is generally the same, but breakthrough times can differ widely from child to child. Some babies are already born with a tooth, others are still completely toothless by their first birthday. For that reason, a delay in terms of months is no cause for concern.
As a general rule, six to eight incisors are visible at the age of one, and by the age of three all milk teeth should have emerged. The complete set of deciduous teeth consists of 20 teeth: 4 incisors, 2 canines and 4 molars each in the upper and the lower jaw.
Teething: What parents should look out for
The process of the first teeth emerging in a baby’s mouth is known as “teething”. Most babies get their teeth without major problems. The imminent arrival of new teeth is generally indicated by increased “drooling” and the baby’s constant desire to chew on hard objects such as a teething ring or a rattle.
Some teething troubles are common when the milk teeth emerge. The inflamed gums are painful, babies are restless, fretful and their sleep is disturbed. A slightly raised temperature or diarrhoea are not uncommon either. Their cheeks are often red and they may suffer from nappy rash. To alleviate the pain of irritated gums, sugar-free teething gels are available in pharmacies, and a teething ring chilled in the fridge may also help. The paediatrician should be consulted if the fever is high or prolonged or in case of other abnormal symptoms.
The emergence of the permanent teeth: the second dentition

Around the child’s sixth birthday, the second dentition begins with the appearance of the first permanent tooth. This is the first molar, also known as the sixth-year molar. Because it emerges behind the last milk tooth without a milk tooth falling out, its eruption often goes unnoticed.
The emergence of the second dentitions proceeds in two stages:
6-8 years:
The first permanent tooth to appear is the molar behind the milk teeth, then the milk incisors become loose and the permanent incisors appear. Often, the milk teeth do not fall out straight away, even though the permanent teeth have already erupted immediately behind (towards the tongue). Thanks to the pressure of the tongue on the new teeth, the milk incisors tend to fall out within a few months. As the new teeth are sized for the adult skull, they appear far too big in the child’s mouth.
10-13 years:
The milk molars now fall out and are replaced by the permanent premolars, and the permanent canines replace the milk ones.
Dental trauma in children – what to do

fracture of the two permanent
central incisors

composite. Despite the exposure of
the pulp (tooth’s nerve), the vitality of
the teeth could be preserved and
root canal treatment avoided.
Dental accidents are particularly common among children and adolescents. While small children often fall or hit their heads when playing, older children and adolescents are mostly involved in sports accidents, e.g. while skateboarding. In most cases milk tooth injuries are relatively harmless, but quick action is required for permanent teeth that are loosened or knocked out. It is important to secure broken tooth pieces, which can often be glued on again. Knocked out permanent teeth are best kept in a tooth rescue box, which is available in the pharmacy. Alternatively, the tooth can also be stored in cold milk. Do not touch the tooth at the root, but at the crown. Please do not waste any time when your teeth are knocked out and see your dentist immediately: replanting is more successful the faster it is done.

tooth rescue box
"Dentosafe"
If your dentist cannot be reached, please contact the dental emergency service responsible for your canton in the event of dental accidents.
Chalky teeth (MIH): When teeth crumble
What is MIH?
Chalky teeth or MIH (Molar Incisor Hypomineralisation) are a relatively common developmental disorder of the permanent teeth, sometimes also the milk teeth, which occurs in 10-15% of all children. Above all, the central permanent incisors (incisors) and the first permanent molars are affected (“cheese molars”). Chalky white or yellow-brown spots are the distinguishing feature of MIH teeth. But the changed tooth enamel is also structurally damaged and not sufficiently resistant: caries can spread quickly on chalky teeth, but the affected teeth can also crumble off when chewing. Another problem with chalk teeth is sometimes extreme sensitivity to touch or temperature, which can cause pain when eating and cleaning.


Causes of MIH:
The cause of this enamel malformation is still unclear. The tooth enamel is formed in the last months of pregnancy and in the first four years of the child’s life. A harmful influence of childhood diseases, medication (antibiotics) or environmental factors is currently being discussed.
How can you recognise MIH teeth?
The experienced paediatric dentist usually recognises at first glance the enamel defects and discoloration of the incisors and molars that are typical for MIH. Sometimes MIH children also show conspicuous enamel malformations in the milk dentition.
Treatment of MIH chalk teeth:
Close dental surveillance of children affected by MIH is particularly important. Because of the risk of caries, toothbrushing at home should be carried out particularly accurately. The dentist can also protect the affected teeth with a fluoride varnish or seal them with resin. If tooth enamel crumbles or flakes off, the tooth is built up with a composite filling. In the case of extensive defects, ceramic crowns may also be necessary.

Treatment of esthetically unpleasing yellow-white- brown spotting and opacities of MIH-teeth in a 18-year old patient. The young woman was distressed by the looks of her front teeth and was ashamed to smile. Using the minimal invasive increment-technique with esthetic composite filling material we were able to remove the multicoloured spots and give her front teeth a beautiful and natural look.
Fighting caries – From he very first tooth
A cavity in the tooth – how does caries develops

Caries (also known as tooth decay) develops as the result of acid-producing bacteria. These bacteria form a sticky coating (plaque) which adheres to the surface of the tooth and cannot simply be removed by rinsing. From sugary foods, the bacteria generate acid which then attacks the hard enamel by dissolving its component minerals such as calcium. In its early stages, caries only appears as a chalky-white spot; the enamel is softened (demineralised), but not yet penetrated. The further progression then sees the appearance of the classic “cavity” in the tooth enamel, and the caries begins to spread in the underlying dentine. Latest at this stage, a filling is needed in order to stop the caries. Pain only appears when the decay is coming close to the dental nerve (pulp). At that stage, root canal treatment often becomes unavoidable.
Parents erroneously assume that caries in milk teeth is not that bad because, after all, they are not yet the “proper teeth”. However, baby teeth are not only there to chew solid food and to enable speech, they also act as place holders for the permanent teeth.
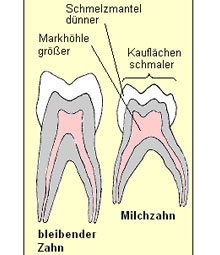
Compared with permanent teeth, the enamel and dentin of milk teeth are thinner and less resistant, while the pulp chamber is larger. For that reason, milk teeth have a lower resistance to caries which can spread quickly and reach the dental nerve, often resulting in tooth ache. The premature loss of a milk tooth due to caries can subsequently lead to a lack of space for the permanent teeth and dental misalignments. For that reason, the primary aim must be to save a milk tooth affected by caries, not to pull it out! Comprehensive information about current options for saving carious milk teeth is available here.
How is caries prevented?
Caries bacteria can be transferred from the mother or carer to the child. In that sense, caries is truly infectious. For that reason, you should never lick the child’s dummy, teat or spoon!
Parents should set an example for their children from the start and demonstrate dental awareness. It is now a known fact that children of parents with good dental hygiene experience far fewer problems with caries than those of parents with bad dental care. One reason for this is the parents’ role model function which children try to copy. But also, the risk of transferring caries bacteria from parents to children is much greater if the parents suffer from bacterial plaque.
Parents must start cleaning baby’s teeth as soon as the first milk tooth appears!
The right diet prevents dental damage.
Fluoride protects children’s teeth.
Cleaning children`s teeth properly

Parents have to start the dental hygiene of their offspring’s teeth as soon as the first tooth appears. Until the age of six, children are not manually able to clean their own teeth systematically; for this reason, it is a job for parents to perform. Once they reach the age of six, children should be motivated to clean their own teeth. However, parents are recommended to follow up by brushing all dental surfaces carefully.
For the first milk teeth, it is sufficient to apply a pea-sized blob of children’s toothpaste to a soft children’s toothbrush and brush the teeth carefully from all sides. Small children are not yet able to rinse and spit out and will thus ingest some of the toothpaste; however, this is not harmful with a small amount of children’s toothpaste.
From the child’s second birthday, teeth should be cleaned twice a day – in the mornings after breakfast and in the evenings before bedtime. Brushing teeth at night should be a fixed part of the bedtime ritual. Afterwards, the child must not consume any more sweets or sugary drinks (juice, milk, ice tea etc.).
From the third birthday, teeth should be cleaned three times a day, about 30 minutes after meal times.
A child’s play approach to teeth cleaning
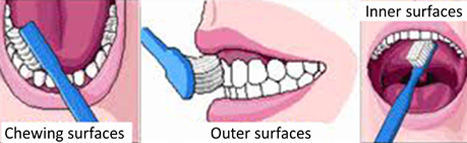
The KAI technique is an easy-to-learn method for cleaning teeth. It ensures that teeth are always cleaned the same way as efficiently as possible without “forgetting” any dental surfaces. The German acronym KAI refers to the order of cleaning: first the chewing surfaces, then the outer surfaces of the teeth and then the inner ones.
The best way for children to learn this technique is by parents showing them and children copying the motions in front of the mirror. But it remains necessary for parents to follow up the children’s solo efforts by brushing their teeth until the children are able to perform this task fully independently (generally by the age of 8 to 10).
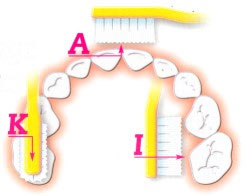
K CHEWING SURFACES: Short back-and-forth brush strokes
A OUTER SURFACES: The teeth are closed and brushing progresses from the middle to the left and right in circular brush strokes
INNER SURFACES: With the mouth open, the inner surfaces of the teeth are wiped from red to white (gum to tooth) as if with a hand brush.
The right toothbrush for children

A child’s toothbrush should have a short thick handle that is comfortable for a child to grip. The head should be short (less than 2 cm) and have as many rounded, rather soft bristles as possible. Natural bristles are quickly colonised by bacteria and thus not suitable for toothbrushes. As a general rule, toothbrushes should be replaced every three months.

Electric toothbrushes for children can help motivate lazy brushers to clean their teeth. It is important that the head is not too big so that all tooth surfaces can be reached. Thanks to the automatic oscillation of the brush, the bacterial plaque is removed very effectively; however, even using an electric toothbrush requires the diligent cleaning of all tooth surfaces in accordance with the KAI technique. Some electric toothbrushes for children have a musical timer with different tunes to “reward” children for diligent brushing.
The right toothpaste for children

The main difference between toothpaste for children up to the age of 6 and adult toothpaste is the reduced fluoride content of the former (500 ppm instead of 1500 ppm). The reason for this is that small children cannot easily rinse and spit, but generally swallow the toothpaste; for the pea-sized blob of children’s toothpaste, this is completely harmless. Furthermore, children’s toothpaste is generally adapted to small children’s taste who would find normal adult toothpaste far too strong. However, children’s toothpaste should not be too sweet or candy-flavoured to avoid the temptation of “snacking”.
From the age of six, junior or adult toothpaste with a fluoride content of 1000-1500 ppm can be used.
Incidentally, children should not be encouraged to rinse their mouths after brushing to ensure that the protective fluoride remains in contact with the teeth for as long as possible.
The right diet
Caries is caused by bacteria fermenting sugar and other carbohydrates in the mouth, thus producing acid which attacks the tooth enamel. Bacteria can feed on the following kinds of sugar:
- Normal granulate sugar (cane sugar, sucrose/saccharose)
- Glucose (dextrose)
- Milk sugar (lactose)
- Fruit sugar (fructose)
Starch, e.g. in potatoes, noodles, rice or bread, can be broken down to sugar and is thus also cariogenic (causing tooth decay), though to a lesser extent than the types of sugar listed above.
The aim of a tooth-friendly diet is to reduce the length of time that carbohydrates and sugar remain in the mouth. Caution: Many foods and drinks contain hidden sugar, e.g. ketchup, muesli bars, milk and chocolate drinks, muesli, cereals, bananas and other types of fruit.

Caries bacteria cannot use sweeteners such as aspartame, cyclamate and saccharin, for that reason, these sugar substitutes are not cariogenic, i.e. they cannot cause caries. Tooth-friendly sweets containing sweeteners instead of sugar bear the “tooth man logo”and the label “tooth-friendly”.
Baby food: the problem is in the bottle

Baby bottle caries:
Massive destruction of milk teeth by caries in a three-year old child caused by constant sucking on sweetened infant tea in a baby bottle. The parents used to give the bottle at bedtime to pacify the child.
This form of caries is also known as the nursing bottle syndrome.
Give a baby water to quench the thirst in between milk feeds. Never give sugary baby tea, sweetened fruit juice, squash, syrup, ice tea or similar in a feeding bottle.
Never give the child a feeding bottle for pacifying or constant sucking while in bed or in the pram, not even with milky drinks.
Get your child used to drinking from beakers and cups as early as possible. Your baby should have stopped using a bottle altogether by his first birthday. Never dunk dummies in sugar or honey.
From infant age:
- Serve sugary dishes only at or immediately after the main meals, not spread across the entire day.
- Serve as few snacks as possible.
- Too many sweets spoil the appetite for healthy food and promotes excess weight.
- Parents need to brush their children’s teeth thoroughly after each main meal.
Our paediatric specialist is happy to advise on the best nutrition for your child.
Fluorides
Fluorides are naturally occurring essential trace elements (flour compounds) that provide proven protection against caries by
- hardening the tooth enamel and safeguarding it from bacterial acid attacks
- inhibiting bacterial growth.
Many foods, particularly fish and crustaceans, contain some fluorides, but not in sufficient quantities for effective caries protection. For that reason, an additional supply of fluoride is necessary. The current recommendations by paediatricians and dentists are:
- Always use fluoridated salt (e.g. salt with iodine and fluoride)
- Use fluoridated children’s toothpaste from the appearance of the first milk tooth
- Use junior or adult toothpaste from the age of six
Preparing the first visit to the dentist

The first impression is important: To make sure that the first visit to the dentist is a positive experience for the child and to establish a relationship of trust, it is important that you as parents take the correct approach. Children are very sensitive to their parents’ fears and emotions. For that reason, choose your words carefully when you talk about the dentist. Avoid any kind of “horror story” and keep quiet about any bad experiences with dentists that you may have had.
Sentences such as “You do not need to be afraid” or “It won’t hurt at all” are bad, because they suggest to the child a possible connection between dentist, fear and pain. Never use the dentist as a threat if your child does not want to clean his teeth.
Prepare your child for the appointment by reading children’s books about visits to the dentist or by play-acting a visit to the dentist using a favourite doll or soft toy. It goes without saying that your child is most welcome to bring the doll or toy along for the visit.
For small children, in particular, it is very important that the visit to the dentist fits in with the normal daily routine. The ideal time for appointments is in the mornings, because children are generally well rested and more receptive and resilient. Avoid appointments at times when the child usually has a nap.
During and after your child’s dental appointment
A sound relationship of trust between your child and the dentist is the basis for successful treatment. To establish such a relationship, the child needs to concentrate on what the dentist is saying. A child cannot listen to two adults at the same time. For that reason, we ask you to support your child with your presence during treatment, but to keep a low profile in communication and leave the dentist to take the lead during the treatment whenever possible.
Praise your child after the treatment! This boosts motivation for the next visit.
Questions and answers
When the first milk teeth have emerged. The main purpose of this first consultation is to advise parents: tips on oral hygiene and nutrition as well as on the avoidance of bad habits such as sucking thumbs can prevent future damage.
As a general rule every six months; in the absence of caries and with generally good oral hygiene, the dentist may well advise on longer intervals.
It is advisable, as there is a form of caries that develops between the teeth without being visible from the outside. For that reason, a small X-ray of the teeth should be taken once a year after the age of three.
Hidden caries developing invisibly in the interdental space is particularly vicious. X-ray is the only way for its early detection before extensive damage is caused. For that reason, dentists now recommend an annual X-ray of the milk teeth once the child has reached the age of three. Modern digital X-ray images require a very low radiation dose and are thus entirely safe.
Try to outwit your child with fantasy and play. The best way forward is to turn teeth cleaning into a ritual. You can sing a particular song while brushing the teeth or recite a poem or tell a story to distract the child. For small children, cleaning teeth while the child lies on the changing table is a proven solution.
IIn the correct dosage, fluorides are very useful and not dangerous. The standard application form (fluoridated toothpaste or fluoridated table salt) is absolutely safe and ensures good protection against caries.
Children should have stopped sucking their thumbs or using a dummy by their third birthday at the very latest. Otherwise they may develop jaw deformations, misalignments of teeth (open bite) or speech impairments. Appeal to your child's sense of pride: explain that he is now to big still to suck thumbs or a dummy, because that is what babies do. Convince your child that the Dummy Fairy has come and taken away the dummy.
That is a common problem. The paediatric dentist will try to introduce the child gently to any treatment. However, there are times when a sedative or laughing gas is needed in order to be able to treat a child. In certain cases - for very small children or children with certain disabilities - the best option is for treatment under general anaesthetic.
If permanent teeth have been completely or partially knocked out, it is vitally important that the tooth (or the section of tooth) is found. Do not touch the root of the tooth but lift it by the crown and keep in a Dentosafe tooth rescue box or alternatively in cold milk. In an emergency, the tooth can also be kept in the mouth underneath the tongue. Go to your dentist immediately (or outside surgery hours to the dental emergency service). Milk teeth that have been knocked out are not reimplanted, because this might cause damage to the permanent teeth. In any case, you should visit the dentist as soon as possible. For your information, your mandatory health insurance or your accident insurance will pay for costs arising from dental injuries. For that reason, it is crucially important to report the injury.
Please contact us by phone or email. We are sure to find an answer to your question.